

Abstract
Background: Hospitalized medically ill patients are at risk for venous thromboembolism (VTE) for at least 45 days after discharge. This observation prompted the MAGELLAN and MARINER trials, which evaluated the efficacy and safety of rivaroxaban for extended thromboprophylaxis. In MAGELLAN, rivaroxaban (10 mg once daily) started in hospital and continued for 35 days was compared with a 10±4 day course of enoxaparin (40 mg once daily) followed by placebo. In MARINER, a 45-day course of rivaroxaban (10 mg once daily for those with creatinine clearance [CrCl] ≥50ml/min and 7.5 mg once daily for those with CrCl 30-<50ml/min) started at discharge was compared with placebo. The goals of this analysis were: (i) to compare rates of VTE (total or symptomatic) and VTE related death and major or clinically relevant bleeding in patients with moderate renal insufficiency (CrCl 30-<50ml/min) and those with normal renal function (CrCL ≥50ml/min), and (ii) to determine if revised criteria for selecting patients for extended thromboprophylaxis are associated with reduced bleeding, particularly in those with moderate renal insufficiency.
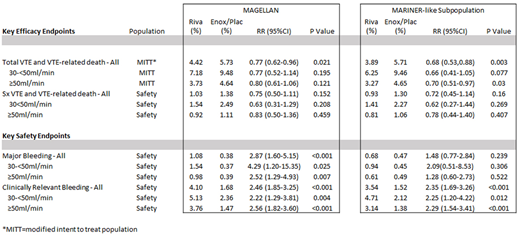
Methods: We evaluated key efficacy and safety outcomes in patients with moderate renal insufficiency and those with normal renal function from days 1 to 35 in the MAGELLAN study and in a MARINER-like subpopulation of MAGELLAN using the criteria defined a priori for patient exclusion used in the MARINER study. These criteria were: 1) active gastroduodenal ulcer within 3 months of randomization or currently symptomatic, 2) any bleeding within 3 months prior to randomization or during index hospitalization prior to randomization, 3) active cancer at randomization, 4) medical history of severe bronchiectasis or pulmonary cavitation, or 5) dual antiplatelet therapy at baseline. These criteria excluded approximately 20% of subjects in MAGELLAN at high risk of bleeding.
Results: The rates of VTE and VTE related death in both the rivaroxaban and enoxaparin/placebo groups were approximately twofold higher in subjects with renal impairment than in those with normal renal function, but the relative risk reduction with rivaroxaban treatment (10mg) compared with enoxaparin/placebo was similar in both renal function subgroups. Rates of major and clinically relevant bleeding in the rivaroxaban group were approximately 50% higher in patients with renal impairment compared with those with normal renal function. In the MARINER like subpopulation, the relative risk reductions for efficacy outcomes were maintained in both renal subgroups, whereas the increase in major bleeding with rivaroxaban was reduced by approximately 50%.
Conclusions: Medically-ill patients with renal impairment given extended thromboprophylaxis are at increased risk for both VTE and major bleeding. Use of the MARINER criteria to exclude patients at increased risk of bleeding appears to reduce the major bleeding risk without compromising the efficacy of 10mg daily of rivaroxaban.
Weitz:Novartis: Honoraria; Servier: Honoraria; Janssen: Honoraria; Ionis: Consultancy, Honoraria; Daiichi-Sankyo: Honoraria; Bristol-Myers Squibb: Honoraria; Boehringer Ingelheim: Honoraria, Research Funding; Bayer: Honoraria. Raskob:Janssen: Consultancy; Bayer: Consultancy; BMS: Consultancy; Daiichi Sankyo: Consultancy; Boehringer Ingelheim: Consultancy; Eli Lilly: Consultancy; Pfizer: Consultancy, Honoraria; Novartis: Consultancy. Spyropoulos:Bayer: Consultancy, Membership on an entity's Board of Directors or advisory committees; Colorado Prevention Center - ATLAS: Consultancy; Portola: Membership on an entity's Board of Directors or advisory committees; Boehringer Ingelheim: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding; Janssen: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding. Cohen:Aspen: Consultancy, Speakers Bureau; Bayer: Consultancy, Speakers Bureau; Boehringer Ingelheim: Consultancy, Speakers Bureau; BMS: Consultancy, Speakers Bureau; Daiichi Sankyo: Consultancy, Speakers Bureau; GSK: Consultancy, Speakers Bureau; Janssen: Speakers Bureau; Medscape: Consultancy, Speakers Bureau; Pfizer: Consultancy, Speakers Bureau; Portola: Consultancy, Speakers Bureau; AbbVie: Consultancy; ACI Clinical: Consultancy; Boston Scientific: Consultancy; CLS Behring: Consultancy; GLG: Consultancy; Guidepoint Global: Consultancy; Leo Pharma: Consultancy; McKinsey: Consultancy; Sanofi: Consultancy; Navigant: Consultancy; ONO: Consultancy; Takeda: Consultancy; Temasek Capital: Consultancy; TRN: Consultancy. Spiro:Bayer: Employment, Equity Ownership. De Sanctis:Bayer: Employment, Equity Ownership. Xu:Janssen Research and Development LLC: Employment, Equity Ownership. Suh:Janssen Research and Development LLC: Employment, Equity Ownership. Lu:Janssen Research and Development LLC: Employment. Lipardi:Janssen Research and Development LLC: Employment, Equity Ownership. Barnathan:Janssen Research and Development LLC: Employment, Equity Ownership.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal